AORTA-iliac occlusive disease
The aorta is the body's largest artery. It carries blood from your heart, down through your chest and abdomen, then splits low down (near your belly button) into two branches – the iliac arteries – that supply each leg.

Aorto-iliac Occlusive Disease
Aorto-iliac occlusive disease is a narrowing or blockage of the iliac arteries – the branches of the aorta that carry blood into your legs. It is a form of peripheral arterial disease (PAD).
It develops when plaque (a build-up of cholesterol and calcium) collects in the artery walls and hardens them – a process called atherosclerosis. As the arteries narrow, less blood and oxygen reach your legs, which can cause pain when you walk. In severe, untreated cases it can lead to sores (ulcers), gangrene, or even loss of a limb, though this is uncommon.
The good news is that it can usually be treated – with lifestyle changes, medication, or a procedure to restore blood flow.

Symptoms
Claudication
The usual first symptom is cramp, ache or tiredness in your buttocks, thighs or calves when you walk, which eases when you rest (called intermittent claudication). As the disease progresses, the pain comes on after shorter distances.
Rest pain
In more advanced disease, you may feel pain in your feet or toes even at rest. Some men also notice erectile dysfunction.
Warning signs that it has advanced:
Severe pain, coldness or numbness in the leg
Sores on the toes, heels or lower legs
Dry, cracked skin that may become infected
Weakened leg muscles
Gangrene (tissue death)
These usually mean the arteries are blocked in more than one place, and need prompt treatment to avoid losing the limb.
Causes
The main cause is atherosclerosis (hardening of the arteries). Things that raise your risk:
Smoking
High cholesterol
High blood pressure
Being overweight
A family history of heart or artery disease
Rarely, inflammation of the artery wall (Takayasu's arteritis, usually in young women) is the cause.
Tests
I start by asking about your symptoms and health, and feeling the pulses in your legs.
Ankle-brachial pressure index (ABPI)
A simple comparison of the blood pressure at your ankle with that in your arm, using a cuff and a hand-held ultrasound (Doppler). A lower ankle reading points to narrowed leg arteries. It confirms the problem but does not show exactly where the blockage is.
Doppler ultrasound (duplex)
A painless scan that shows blood flow and pinpoints which arteries are narrowed.
Angiography
Contrast dye and x-rays map the exact site and pattern of the blockages, usually when a procedure is being planned.
Treatment Options
Lifestyle Changes
Stopping smoking is the single most important thing you can do – tobacco directly damages your arteries.
A structured walking programme is the most effective non-surgical treatment for claudication: walking regularly, ideally a supervised programme most days of the week, trains your legs to walk further with less pain. Keeping to a healthy weight and eating a low-fat, high-fibre diet also help slow the disease.
If you have diabetes, good blood-sugar control and careful foot care are important, because reduced feeling in the feet makes sores more likely. A podiatrist can help.
Medication
Medication supports these measures rather than replacing them. An antiplatelet (aspirin or clopidogrel) lowers the risk of clots, and a statin lowers cholesterol; your blood pressure and blood sugar are also treated to protect your arteries. A medicine such as cilostazol (or pentoxifylline) may modestly improve how far you can walk.
Intervention
If the disease is severe, or does not improve with the steps above, a procedure may be needed to restore blood flow. The best option depends on where the blockages are and how extensive they are.
Forms of Intervention
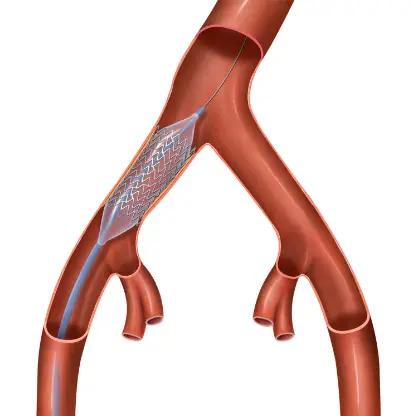
Angioplasty with or without stent
A thin tube (catheter) is passed from an artery in your leg to the narrowed area. A small balloon is inflated to widen the artery, and a small mesh tube (stent) may be left in place to hold it open. Blood then flows more freely.
Endarterectomy
Through an incision in your leg or groin, I remove the plaque from the lining of the artery, leaving it open and restoring blood flow.
Bypass surgery
A fabric tube (graft) is used to route blood around the blocked section – for aorto-iliac disease, usually a Y-shaped graft from the aorta to the arteries in each groin. It is a durable operation, and most grafts are still working well many years later.
References
European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on Asymptomatic Lower Limb Peripheral Arterial Disease and Intermittent Claudication. Eur J Vasc Endovasc Surg, 2024.
Society for Vascular Surgery Clinical Practice Guideline on the Management of Intermittent Claudication: Focused Update. J Vasc Surg, 2025.



 Postoperative Protocol - Aorta-Bifemoral Bypass
Postoperative Protocol - Aorta-Bifemoral Bypass Patient Roadmap for Aortabifemoral Bypass Surgery
Patient Roadmap for Aortabifemoral Bypass Surgery Aorta-Bifemoral Bypass - Discharge Protocol
Aorta-Bifemoral Bypass - Discharge Protocol Aorta-Bifemorale Omleiding - Ontslagprotokol - Afrikaans
Aorta-Bifemorale Omleiding - Ontslagprotokol - AfrikaansOur Services
Arterial Procedures
Standard open arterial surgical procedures to repair aorta aneurysm and / or reconstruct blood flow to the lower extremities.
Open aorta aneurysm repair
Aorta-bifemoral bypass
Iliofemoral bypass
Endarterectomies
Endovascular Procedures
Less invasive percutaneous procedures to repair blood flow through the aorta to intestines, organs and extremities.
Mesenteric artery angioplasty
Renal artery angioplasty
Aorta angioplasty
Iliac artery angioplasty
Subclavian artery angioplasty
Hybrid Procedures
Combined endovascular and open surgical procedures to repair abdominal aorta aneurysms, thoracic aneurysm or to improve blood flow to the extremities.
Endovascular abdominal aorta aneurysm repair
Endovascular thoracic aorta aneurysm repair
If you have any problems with any of these conditions, please contact your General Practitioner, or your Vascular Surgeon. If you live in Pretoria and have not seen a Vascular Surgeon before, you are more than welcome to contact my rooms for a formal consultation.
The purpose of this web site is to offer Dr Weir’s patients and their families access to information regarding vascular disease in general as well as specific information on certain disease processes. The information on this site does not necessarily apply to all patients with the same diagnosis. If you are not a patient of Dr Weir, please do not regard the information on this website as a substitute for a thorough assessment by a qualified Vascular Surgeon. If in doubt, consult your doctor.
If you are experiencing a medical emergency, phone us. If you are not able to get through or if we are not available, please visit your nearest casualty department.
Contact us
Tel: 012 335 8651 · Email: [email protected]